Coroner finds missed lithium checks delayed treatment before Wendy Gorrie’s death
Wendy Gorrie showed all the signs of lithium toxicity – but her levels weren’t checked when she was admitted to hospital.
In November 2024, the 66-year-old was taken to Palmerston North Hospital after she fell and hurt her hip.
She was on a number of medications, including lithium, which she continued to take while in hospital.
But three weeks into her stay she regressed, becoming increasingly agitated, confused, shaky and unco-operative.
It wasn’t until she collapsed and suffered seizure-like movements that her lithium levels were checked, and she was found to have lithium toxicity.
By then she had developed pneumonia and cognitive impairment.
She died in the hospital’s intensive care unit on December 11, 2024.
In a report released today, Coroner Rachael Schmidt-McCleave found there were a number of instances when hospital staff should and could have checked Gorrie’s lithium levels, as she showed signs of toxicity.
MedSafe recommends lithium levels are checked every three months, but Schmidt-McCleave noted Gorrie’s had not been checked for seven.
“Although I am unable to say with certainty that an earlier check would have prevented Ms Gorrie’s death, I do find that Ms Gorrie’s treatment for lithium toxicity was delayed because of a failure by all who treated her to check her levels earlier,” she said.
“I consider it possible that Ms Gorrie’s progression to collapse, pneumonia, and cognitive impairment could have been averted had a lithium level check been undertaken.”
Gorrie lived in Levin with her mother, Joyce Taylor.
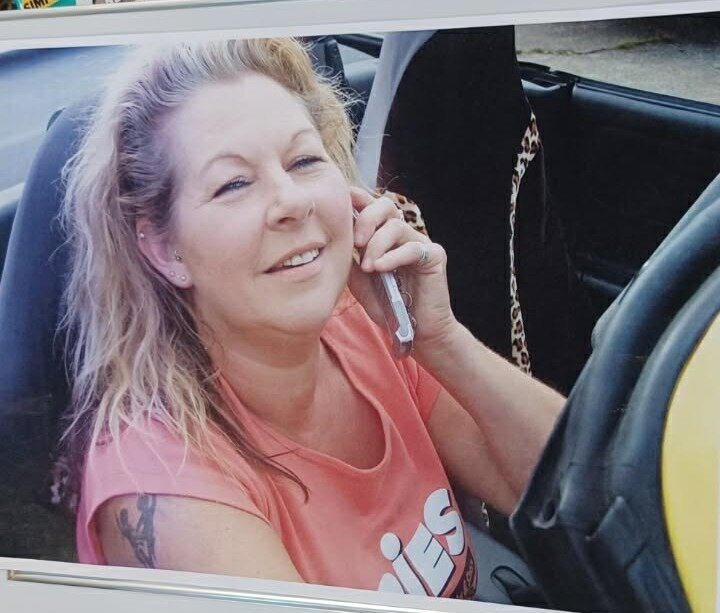
Taylor, now 90, told NZME Gorrie was a “bubbly, happy, lovely,” daughter.
“She’s just a happy person, everybody loved her.”
Taylor said she didn’t visit Gorrie in her final week because she’d caught a cold and didn’t want to make her sicker, so did not get to say goodbye.
“She just went for a week because she had a fall, but she didn’t come out.
“All we want to do is see that this never happens to anybody else.”
Gorrie took prescription lithium
Gorrie was prescribed a number of medications including lithium 400mg daily, venlafaxine 300mg daily, olanzapine 10mg at night, and olanzapine 300mg depot injection every three weeks.
Lithium is a drug that is used as a mood stabiliser. It is usually excreted via the kidneys and can have side effects that particularly affect the kidneys, thyroid gland, and brain.
On November 16, 2024, she was taken to Palmerston North Hospital’s Emergency Department by ambulance with right hip pain.
She had reportedly lost her balance the previous day while walking with her walking frame and had landed on her left buttock and was unable to bear weight on her right leg.
Gorrie’s mother also reported that she seemed more confused than normal.
No fracture was seen on X-rays but Gorrie was admitted overnight with a view to discharge her once she could mobilise.
On the evening of November 16, 2024, Gorrie was described as being confused and disoriented, unco-operative, and unable to stand without assistance.
She was given her usual medications, including 400mg lithium as well as paracetamol for the pain.
The next day, Gorrie was noted to be mildly confused, shaky, and unco-operative.

It was noted that she had acute kidney injury, attributable to dehydration, as indicated by a rise in her creatinine level from a normal level of 85 umol/L at admission to 112 umol/L later in the evening.
There was no record of a lithium blood level being taken at this time.
On December 6, three weeks into her hospital stay, she collapsed and an emergency call was issued at 9.45pm.
Gorrie had developed a reduced level of consciousness, “jerky seizure activity” for three minutes, muscle spasms, muscle rigidity, tachycardia, rapid breathing and reduced oxygen saturations.
A blood gas showed lactic acidosis with hypoxia, a non-specific indicator of hypoxia and/or acute shock.
She was given oxygen via a mask, adrenaline, salbutamol and ipratropium for wheeze/asthma.
The initial thought was aspiration with hypoxia, with or without an acute seizure. A broad-spectrum antibiotic was administered to cover the possibility of pneumonia but an X-ray showed no definite pneumonia.
At 10pm, a lithium level was requested. It was toxic at 1.90mmol/L. The therapeutic range is 0.6-0.8mmol/L. She was admitted to the ICU.
The lithium level was the first laboratory record of a lithium level since May 2024.
“In this regard, I note that the initial report by the Te Whatu Ora specialist intensivist that I received referred to Ms Gorrie having normal lithium levels on admission to hospital, but there are no records in the evidence before me of a lithium test before December 6, 2024,” Coroner Schmidt-McCleave said.
“I consulted with Te Whatu Ora about this, and Te Whatu Ora confirmed that the specialist interventionist had made a mistake by initially advising my inquiry that the lithium level on admission was normal.”
Gorrie’s renal function and lithium level slowly normalised, but she continued to have problems with severe agitation and confusion.
Additionally, her respiratory function continued to worsen despite the antibiotic treatment, with her developing bilateral pneumonia.
Gorrie was given a poor prognosis and was transitioned to palliative care. She died on December 11, 2024.
Staff failed to check lithium levels
Te Whatu Ora Health NZ MidCentral commissioned a Serious Adverse Event Review (SAER).
It found Gorrie’s lithium levels in 2023 were taken approximately on a six-monthly basis.
Her lithium level was taken on May 3, 2024, which was normal at 0.4. When she was tested while she was in hospital, it had reached a toxic level.
Signs of toxicity vary and may include muscle weakness, lethargy, impaired balance, lack of co-ordination, tremor of the extremities and lower jaw, twitching, agitation, altered speech, disorientation, psychosis, drowsiness and seizures.
A check of Gorrie’s lithium levels on the day of her admission to hospital “would have been a reasonable thing to do,” the review report said.
The SAER recommended Gorrie’s case review be shared with the “key learning to ensure timely lithium levels to be checked in either the ED or Medical ward for patients on lithium who present medically unwell”.
In the Coroner consultation process, the Chief Medical Officer of Te Whatu Ora MidCentral, Dr Claire Hardie, added comment addressing the recommendation to remind general medicine senior medical officers of the need to ensure timely lithium level monitoring for patients on lithium who present as medically unwell.
Hardie told the coroner that it had been communicated to the teams and an anonymised case review for learning purposes was being organised.
The coroner said evidence showed Gorrie was likely experiencing lithium toxicity before she presented to hospital.
A support worker reported that she had noticed decline over the last several weeks and Gorrie’s mother reported that Gorrie had declined in the six weeks prior to her admission, with falls, reduced mobility and cognitive decline.
A GP record on November 15, 2024 stated: “seen due to deterioration in her cognition and jerks of all her body”.
“I consider it possible that Ms Gorrie’s progression to collapse, pneumonia, and cognitive impairment could have been averted had a lithium level check been undertaken,” Coroner Schmidt-McCleave said.
Brianna McIlraith is a Queenstown-based reporter for Open Justice covering courts in the lower South Island. She has been a journalist since 2018 and has had a strong interest in business and financial journalism.